

The conventional fashion to treat dysplasia was with the use of bone graft to make up for the deficient socket. While this appears logical from a layman standpoint it lead to an unacceptable failure rate in 6-7 years of over 40 % in some series.
The modern uncemented sockets have revolutionized the management of dysplasia. The key is to avoid a structural bone graft and ensure excellent host bone contact. This will ensure long term success as the modern uncemented sockets will ensure bonding (Osteointegration) with the bone if host bone contact and primary stability is optimal.
This is achieved by using the modern concepts of a judicious high hip centre, subtle medialisation and special technique of reaming which we have developed in our unit.
We have not had a single case of socket failure in dysplasia over the last 10 years after we adopted this technique.


Dysplastic hips on the femoral side have the problems of abnormal rotation (increased anteversion), increased angle of neck (coxa valga) and decreased width of the pelvis (low offset). These mechanical issues make it a difficult proposition to manage with standard implants.
If these changes are significant, then a modular implant known as S-Rom is critical. With these implants the surgeon is able to factor in all these biomechanical issues and an excellent outcome can be obtained. Pictures show the modular stem and the long neck for getting the biomechanics correct.
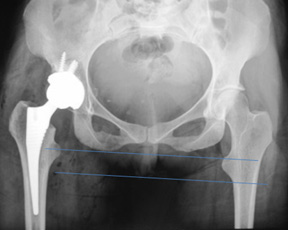
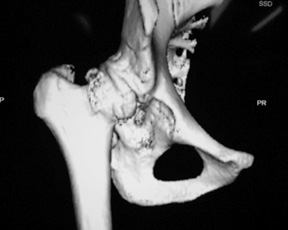
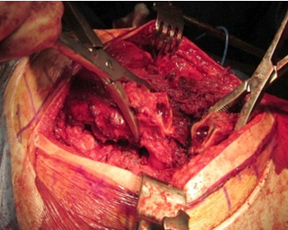
In this patient if one does the traditional method of reconstruction it is obvious that a huge structural graft is required. This disadvantage of this method of reconstruction is that the long-term success of the procedure is linked to the success of the graft which is unpredictable. The modern method of reconstruction has been done with a judicious high hip centre in combination with a wear resistant Delta Ceramic on Delta Ceramic (CoC) bearing. Note that the limb length has been restored with suitable compensation on the femoral side.


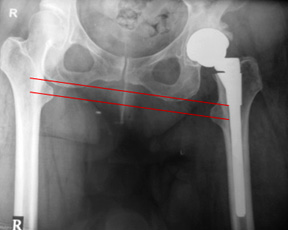

In this patient if one does the traditional method of reconstruction it is obvious that a huge structural graft is required. This disadvantage of this method of reconstruction is that the long-term success of the procedure is linked to the success of the graft which is unpredictable.
The modern method of reconstruction has been done with a judicious high hip centre in combination with a wear resistant Delta Ceramic on Delta Ceramic (CoC) bearing. Note that the limb length has been restored with suitable compensation on the femoral side.


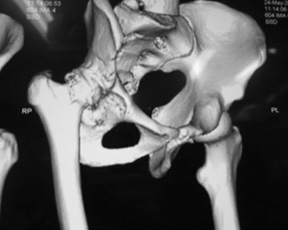
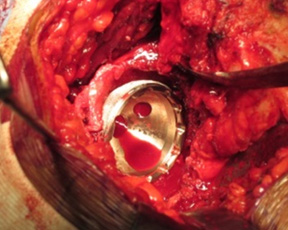
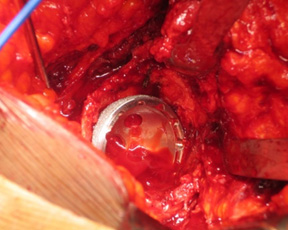
In this example the same features are demonstrated but the dysplasia is of a much higher degree. The major advantage of this technique is the fact that the cup is seated at a place where the best bone stock is available.
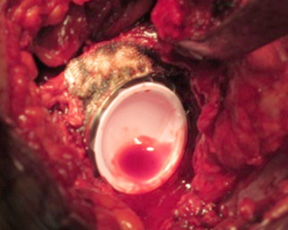
This has huge long-term favourable implications. Wear resistant bearings like CoC are preferred for these young patients with dysplasia. One can see the excellent cover is achieved with outstanding host bone contact in spite of a poorly developed socket . This is possible when a PIAS (Posteroinferior-Anterosuperior) technique of reaming developed by Dr. Bose is used.


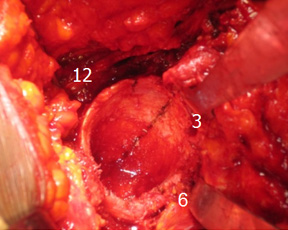

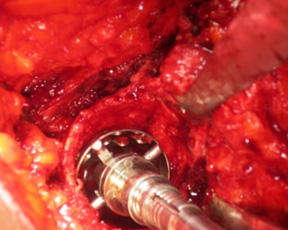
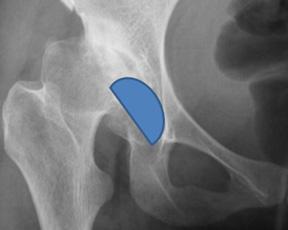
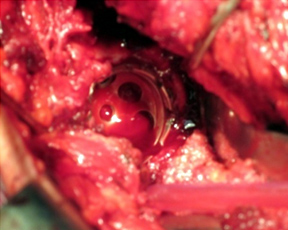
The new technique of reaming is known as dysplasia cup method of PIAS reaming technique. It is traditional understanding that the lack of socket development is superior or in the 12 Oclock position of the socket. This was found to be inaccurate when one does the BHR dysplasia cup. The screws of the dysplasia cup engaged the bone in the 1.30 position for the right hip and 11.30 for the left hip.
This led Dr. Bose to the development of the dysplasia cup method of reaming or the PIAS technique (Post-inf to Ant-sup). By adopting this technique one can get very good to excellent cover in all dysplastic sockets as demonstrated by this case example. This technique has revolutionised the concept of mgmt of dysplastic sockets in our unit. Morcellised bone graft covered with Surgicel is used and a structural bone graft is avoided.
We have a very large experience of dealing with Crowe 4 dysplasia with the S-Rom system.
We have outstanding and predictable results with the Sub-trochanteric shortening osteotomy which is a technically complex procedure to perform.






Surgery for Protrusio

Subtrochanteric shortening osteotomy
Post acetabular fracture surgery

Fused hip take down surgery
Extended trochateric osteotomy
Deltamotion Rationale & Surgical Demo 1
Deltamotion Rationale & Surgical Demo 2

Deltamotion Rationale & Surgical Demo 3

Birmingham Hip Resurfacing Surgery Part 1

Birmingham Hip Resurfacing Surgery Part 2

Birmingham Hip Resurfacing Surgery Part 3

Dr. Vijay C. Bose
Joint Director & Consultant Orthopaedic Surgeon
Hip, Knee and Shoulder
SRM Institutes of Medical Sciences (SIMS)
Vadapalani, Chennai, India
Copyright © 2013 - All Rights Reserved - Dr. Vijay C. Bose
Powered by Deltaprosystems