

AVN is a very confusing condition for patients and doctors as it is very variable amongst different individuals. For some patients , symptoms are so severe as to make them completely crippled. While in other patient symptoms are so mild that the condition goes unnoticed and picked up when x-rays or scans are done for the spine etc.
This disparity may be present amongst two hips in the same patient.
Thus the natural history of the disease in a particular patient is so varied and unpredictable.
This is the reason as to why the efficacy and results of any bone conserving non arthroplasty option in AVN is very difficult to gauge.
If a particular option is done for a patient with a good natural history then the procedure seems successful though the patient may be doing well due to the favourable natural history. The reverse may also be true when a particular procedure may branded useless when it fails in a particular patient who has a very poor natural history.
Thus the suggested treatment options can be so confusing and a surgeon has to deal with a large number of patients so as he can advise the right option for the patient. Dr. Bose has now managed more than 950 patients with AVN over the last 14 yrs. It is important to keep in mind that all patients with AVN do not need surgical intervention.



The treatment options of various stages of AVN is dramatically different.
Fortunately Good medical therapy is now available and this can provide excellent relief for many patients.
Core decompression and some form of bone grafting has been used by surgeons over the last 30 yrs with varied success rates. The reason for the variation is again the natural history of the disease per se. However the overall rate of performing this surgery has declined over the years and is used much less frequently in the recent years. It is now plainly obvious that not all patients with early AVN will benefit from this procedure . However it still has a role is a small sub group of patients. Coming to a decision as to whether core decompression will benefit a particular patients is a difficult task and the rate of coming to correct decision is proportional to the experience of the surgeon with AVN.
Unfortunately there has been an unjustified overuse of the Stem Cell Treatment for AVN. Intuitively stem cell treatment for any medical disorder is very appealing from a patient perspective as it carries an image of becoming new again without any intervention. This is far from the truth and the harsh reality is that the results of stem cell treatment has not lived up to the hype and clinicians are getting increasingly skeptical.
That being said, stem cell therapy has a small role in AVN in the very carefully selected patient.



The intrinsic problem with any kind of biologic procedure is the fact that though we see the bone changes in the x-ray , it is very important to keep in mind that there is a cartilage failure that may be actually more important. Bone grafting obviosely cannot take care of cartilage fail.
Now there is gen. consenus that high profile bone grafts or osteotomy or implants which compromises a future hip arthroplasty must not be done in early AVN.

AVN patients are invariably young and active patients and the prime of their lives and the surgeon has to keep this in mind when offering solutions. Getting rid of the pain for a few years is a very myopic way of looking at the problem. The surgeon must have a clear plan to cater to the patients activity level and to choose options that would lend itself to further surgery if required . This is of vital importance and this differentiates hip and knee replacement surgery in India/ Asia. Knee replacement surgery is generally done for the older relatively inactive patients and thus the implant choice and surgical expertise is not as critical as hip reconstructive surgery in the younger active patient.
High profile implants which are difficult to revise must not be used in young and active patients.

Essentially 3 implants satisfies the needs for the young and active AVN patients.
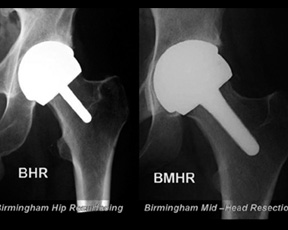
These are BHR / BMHR / Deltamotion
Unlike the western population hip arthritis occurs in young patient in India/Asia. Hence conserving bone becomes crucial. The BHR (Birmingham Hip Resurfacing) and BMHR (Birmingham Mid Head Resection) prosthesis is specifically developed for younger and more active patients.
AJRI has experience of over 2000 BHR/BMHR procedures which makes it the largest volume centre in Asia. In addition, the centre has the largest experience of this procedure for avascular necrosis of hip in the world.


Traditional THR is characterised by 3 important disadvantages:
The Deltamotion eliminates these 3 weak links by providing.
AJRI surgeons have developed the surgical technique for ideal implantation of Deltamotion.


Surgery for Protrusio

Subtrochanteric shortening osteotomy
Post acetabular fracture surgery

Fused hip take down surgery
Extended trochateric osteotomy
Deltamotion Rationale & Surgical Demo 1
Deltamotion Rationale & Surgical Demo 2

Deltamotion Rationale & Surgical Demo 3

Birmingham Hip Resurfacing Surgery Part 1

Birmingham Hip Resurfacing Surgery Part 2

Birmingham Hip Resurfacing Surgery Part 3

Dr. Vijay C. Bose
Joint Director & Consultant Orthopaedic Surgeon
Hip, Knee and Shoulder
SRM Institutes of Medical Sciences (SIMS)
Vadapalani, Chennai, India
Copyright © 2013 - All Rights Reserved - Dr. Vijay C. Bose
Powered by Deltaprosystems